
Knee osteoarthritis is one of the most common causes of chronic pain and limited mobility. Many people are told that medications, steroid injections, or even joint replacement surgery are their only options. But advances in regenerative medicine are changing that story.
In recent years, platelet-rich plasma therapy (PRP) has gained attention as a non-surgical treatment for knee osteoarthritis. PRP uses your own blood-derived growth factors to reduce inflammation and support joint repair. Other commonly used treatments include hyaluronic acid injections, corticosteroid shots, and anti-inflammatory medications. But which option actually provides the most lasting relief?
A new clinical study published in 2025 directly compared PRP, hyaluronic acid, corticosteroids, and NSAIDs for moderate knee osteoarthritis. The results offer valuable insight for anyone seeking alternatives to knee replacement surgery. Below, we break down what the research found and how Regenexx Cayman’s advanced PRP and cell-based procedures build on these findings to deliver next-level regenerative care.
Summary
This 2025 retrospective cohort study compared four common knee-osteoarthritis (OA) treatments: platelet-rich plasma (PRP), hyaluronic acid (HA), corticosteroids (CS), and non-steroidal anti-inflammatory drugs (NSAIDs). Researchers analyzed 205 knees in 150 patients with moderate (Kellgren–Lawrence grade 2–3) OA. Over 6–12 months, pain (VAS scale) and function (WOMAC index) improved in all groups—but PRP achieved the strongest, most durable gains. Patients receiving PRP showed a 3.2-point VAS reduction and 20-point WOMAC improvement, with over 90% reaching clinically meaningful improvement. HA provided moderate, consistent benefit; corticosteroids offered quick but short-lived relief; and NSAIDs produced minimal change. Radiographic progression was lowest in PRP and HA groups. No serious adverse effects occurred. Obesity and more advanced OA reduced treatment benefit. Overall, PRP and HA appear safest and most effective for long-term knee OA management, while CS and NSAIDs should be reserved for short-term symptom control.
Pain Reduction (VAS Decrease)
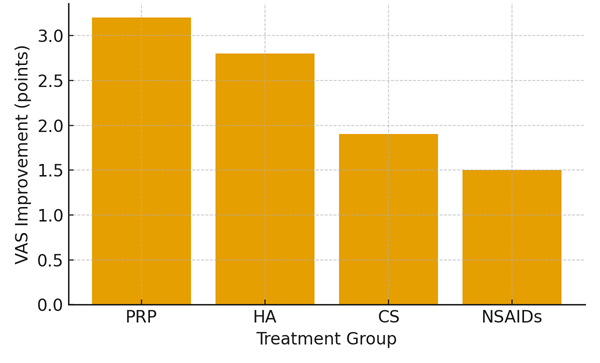
Figure 1. Mean change in VAS pain scores after treatment. PRP produced the greatest improvement, followed by HA, corticosteroids, and NSAIDs.
Functional Improvement (WOMAC Decrease)
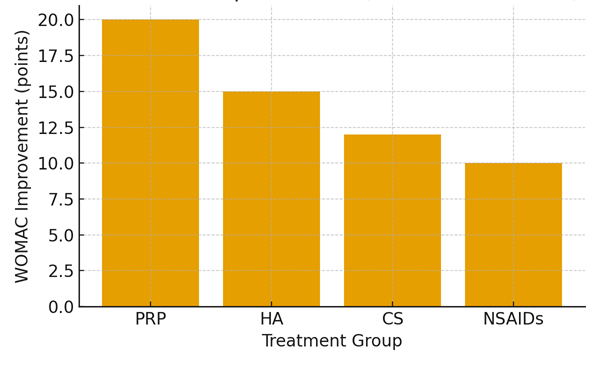
Figure 2. Mean change in WOMAC scores indicating functional improvement. PRP and HA demonstrated the most consistent long-term benefits.
Key Clinical Outcomes Summary
| Treatment | VAS Change | WOMAC Change | VAS MCID (%) | WOMAC MCID (%) |
| PRP | -3.2 | -20 | 91.7% | 88.3% |
| HA | -2.8 | -15 | 86.7% | 83.3% |
| CS | -1.9 | -12 | 71.1% | 66.7% |
| NSAIDs | -1.5 | -10 | 57.5% | 55.0% |
Detailed Discussion and Clinical Implications
Knee osteoarthritis (OA) is one of the most common causes of pain and disability worldwide. Millions of adults struggle daily with stiffness, swelling, and mobility loss that limits work, exercise, and quality of life. Over time, worn cartilage and chronic inflammation worsen the damage—making early, effective treatment essential.
A 2025 study in Medicine journal by Gökçeoğlu et al. directly compared four frequently used therapies: platelet-rich plasma (PRP), hyaluronic acid (HA), corticosteroids (CS), and non-steroidal anti-inflammatory drugs (NSAIDs). The findings shine new light on which approaches truly deliver long-term relief—and which may only offer temporary comfort.
Researchers evaluated 205 knees in 150 patients (ages 40–70 years) with moderate (KL grades 2–3) OA. All received one of the four treatments and were monitored for 6–12 months using validated pain (VAS) and function (WOMAC) scores.
Results showed PRP produced the most significant and lasting improvement, with an average VAS reduction of 3.2 points and WOMAC decrease of 20 points. HA also showed reliable results (−2.8 VAS, −15 WOMAC), while corticosteroids worked quickly but declined by month 6. NSAIDs offered the least improvement and had the highest adverse event rate.
Importantly, non-obese patients and those with milder OA responded better to PRP and HA, highlighting the value of early intervention. No serious adverse events were reported across any group.
These findings align with OARSI and AAOS recommendations favoring PRP and HA over repeated corticosteroid or NSAID use. Regenexx procedures go beyond traditional PRP by using lab-processed platelet lysate and bone marrow concentrate to precisely deliver growth factors and regenerative cells, potentially extending symptom relief and protecting joint structure.
If you’ve been told joint replacement is your only option, research like this shows that biologic interventions can offer a safer, less invasive alternative.
Could your own platelets and cells hold the key to regenerating your joint – without surgery?
Contact Regenexx Cayman to learn how advanced PRP and stem cell-based procedures can help restore function and relieve chronic knee pain.
References
1. Gökçeoğlu YS et al. Medicine. 2025; 104:40 (e44929). doi:10.1097/MD.0000000000044929.
2. Bannuru RR et al. Osteoarthritis Cartilage. 2019;27:1578–89.
3. Laudy AB et al. Br J Sports Med. 2015;49:657–72.
4. Gao J et al. Arch Orthop Trauma Surg. 2024;144:3947–67.
5. Luo P et al. Pain Res Manag. 2020;2020:7587936.
6. Kamada K et al. Asia Pac J Sports Med Arthrosc Rehabil Technol. 2024;38:43–8.
7. Regenexx Cayman Clinical Protocols Overview (2024).